Functional Free Muscle Flap
Individuals with facial paralysis that has been left untreated for two or more years often experience scarring of the facial muscles and subsequent loss of the area's chemical messaging system, producing atrophied muscle that can no longer contract.
Microneurovascular muscle transplantation (free muscle flap) is a smile restoration procedure often suited for individuals with absent facial muscles or with facial muscles that have undergone irreversible atrophy. For example, functional free muscle flap can be beneficial for patients whose facial muscles have been removed during tumor excision or damaged by trauma. In congenital cases of facial paralysis, such as Moebius Syndrome or Craniofacial Microsomia, underdeveloped facial muscles can also require free muscle flap for smile restoration.
Technique
The functional free muscle flap technique involves transplanting an expendable segment of muscle and its associated nerve to the cheek for smile restoration. The gracilis is the most frequently utilized muscle at the Center for Facial Paralysis Surgery and Functional Restoration, although the pectoralis minor, serratus anterior and latissimus dorsi muscles can be employed in certain situations. The gracilis muscle is a thin, flat muscle situated along the inner thigh and is preferred for several functional and cosmetic reasons. The gracilis free muscle flap can be harvested through a well-concealed, limited incision in the upper, inner thigh that is covered by shorts and summer wear.
Fortunately, several other thigh muscles perform the same function as the gracilis muscle. This functional overlap has permitted transplantation of the gracilis muscle while producing limited or no impairment in the thigh and leg. Most patients resume their regular exercise programs and sports activities several months after surgery.
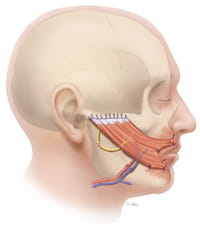
The procedure is initiated by creating a face lift-style incision in front of the ear that is extended below the angle of the jaw. In a fashion similar to a face lift, the skin and fat are lifted from the cheek, creating a pocket to accept the muscle transplant.
The set of blood vessels that will later be used to restore circulation to the transplanted gracilis muscle are identified. Attention is now focused on finding a nerve to provide electrical impulses and motor power to the muscle transplant.
The motor nerve branch to a local chewing muscle is frequently used in this procedure (masseter nerve). The masseter nerve provides strong neural input and allows for the reconstruction to be achieved in a single stage. While biting down is initially required to produce a smile, with practice it is possible to adapt and learn to smile in an almost spontaneous manner.
The set of blood vessels that will later be used to restore circulation to the transplanted gracilis muscle are identified. Attention is now focused on finding a nerve to provide electrical impulses and motor power to the muscle transplant.
The motor nerve branch to a local chewing muscle is frequently used in this procedure (masseter nerve). The masseter nerve provides strong neural input and allows for the reconstruction to be achieved in a single stage. While biting down is initially required to produce a smile, with practice it is possible to adapt and learn to smile in an almost spontaneous manner.
The contralateral, undamaged facial nerve is another possible donor nerve. Nine months to one year prior to the muscle transplant, a long nerve graft spanning the face is placed and connected to redundant branches of the undamaged facial nerve.
Over time the nerve fibers grow across the graft and transmit signals much like a telephone wire. The signal provided by the cross face nerve graft can produce a truly spontaneous, effortless smile but it is frequently weaker than those created by the masseter nerve.
After the recipient nerves and blood vessels in the cheek are identified, a segment of the gracilis muscle and its associated blood vessels and nerve (obturator nerve) are removed from the inner thigh. The muscle is now transferred to the face and secured with stitches to the corner of the mouth and in front of the ear.
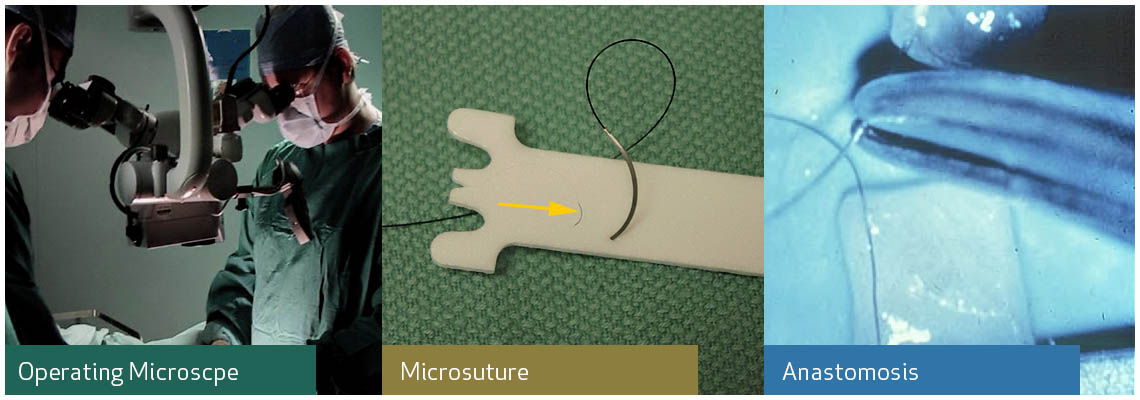
Utilizing an operating microscope and stitches that are finer than a hair, the blood vessels in the cheek are connected to vessels in the transplanted muscle to restore its circulation (microvascular anastomosis). A microsurgical nerve repair is now performed, connecting the motor nerve of the free muscle flap to the masseter nerve or previously placed cross face graft. The incisions are then closed with plastic surgery techniques to maximize the aesthetic outcome.
Over time the nerve fibers grow across the graft and transmit signals much like a telephone wire. The signal provided by the cross face nerve graft can produce a truly spontaneous, effortless smile but it is frequently weaker than those created by the masseter nerve.
After the recipient nerves and blood vessels in the cheek are identified, a segment of the gracilis muscle and its associated blood vessels and nerve (obturator nerve) are removed from the inner thigh. The muscle is now transferred to the face and secured with stitches to the corner of the mouth and in front of the ear.
Utilizing an operating microscope and stitches that are finer than a hair, the blood vessels in the cheek are connected to vessels in the transplanted muscle to restore its circulation (microvascular anastomosis). A microsurgical nerve repair is now performed, connecting the motor nerve of the free muscle flap to the masseter nerve or previously placed cross face graft. The incisions are then closed with plastic surgery techniques to maximize the aesthetic outcome.
Recovery
A 5-7 day period of hospitalization is typically required for free muscle flap procedures. The first 48 hours are spent in a specialized unit to allow for intensive monitoring of the transplanted muscle with a hand held microphone (Doppler).Once transferred to the regular ward most patients have limited discomfort and walk rapidly.
After discharge from the hospital patients are encouraged to drink lots of fluids, avoid pressure to the treated side of the face and refrain from exertional activities for 6-8 weeks. No facial movement is anticipated for a period of six months while the donor nerve grows into the transplanted muscle.
Once a smile appears, electrical stimulation therapy and a home exercise program is often initiated. Over a several year period a process of learning and adaptation occurs frequently improving the quality, strength and control of the reconstructed smile.
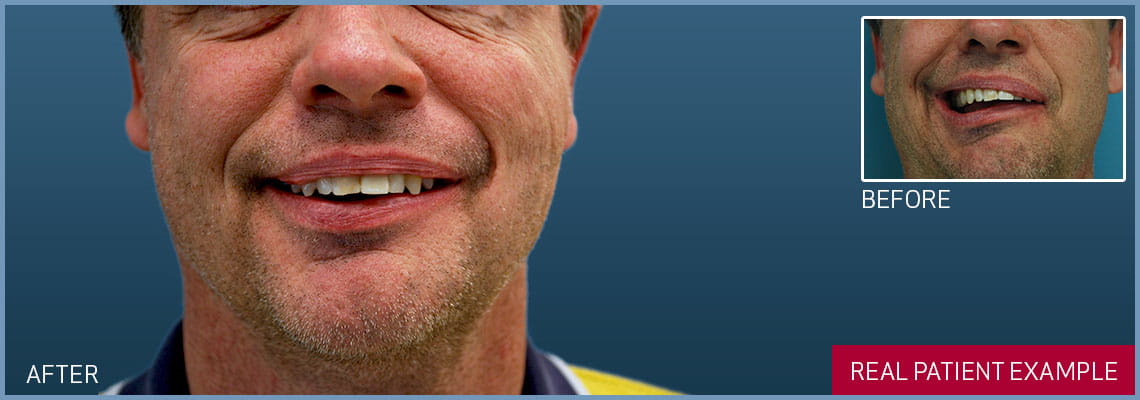
FUNCTIONAL FREE MUSCLE FLAP

Patient exhibited an incomplete resolution of Bells palsy with persistent left facial weakness. After Surgical Smile Restoration (cross face nerve graft and free gracilis muscle flap), the patient is able to smile again.
real patient case studies
Learn how facial paralysis surgery and functional restoration can help you.